Relevance: Anaemia is a condition in which a person lacks enough healthy red blood cells to carry adequate oxygen to his/her body tissues. Having anaemia, also referred to as low hemoglobin can make the person feel tired and weak. There are many forms of anaemia, each with its own cause. Athletes can develop anaemia, most commonly caused by iron deficiency. Iron deficiency is the foremost cause of true anaemia. True anaemia curbs athletic performance, but nonanaemic iron deficiency does not. Range: The range of RBC leading to anaemia: For Men: below 4.3 million cells/mcL, For Women: below 3.9 million cells/mcL
Purpose: To investigate the blood specimens of the athletes and check the blood count for anaemia by using complete blood count (CBC) method. The objective of this research is to study the blood tests of athletes in the Odesa Region, South of Ukraine
Materials and Methods: The methods used in this research will be lab methods like the general blood test and the materials used are syringe, alcohol swabs and cotton, bandages, test tubes (EDTA and plain tube), microscope slides, staining reagents, hematology analyzer. The study was conducted on the basis of “Odesa National Medical University with Physical Rehabilitation and Sports medicine department in association with various regional hospitals.” We analyzed specimens of various athletes during the year 2021 from various regions of Odesa. The total no. of athletes on whom the investigations were conducted were 2050.
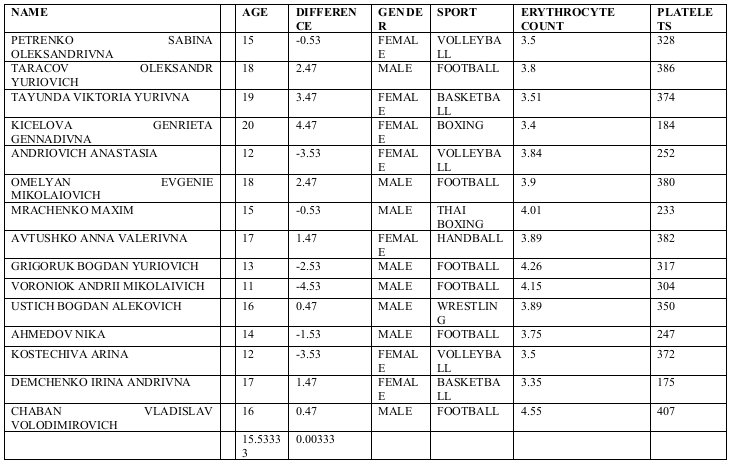
Result: Out of the total no. of athletes, 15 athletes who were diagnosed with iron deficiency anaemia belonged to following category of sports; Boxing (1case), Muay Thai (1 case), Wrestling (1 case), Basketball (2 cases), Football (7 cases), Volleyball (3 cases), Handball (1 case) where football had 46.7% of the cases.
Conclusion: The research showed that 0.73% of total athletes investigated were diagnosed with iron deficiency anaemia in the Odesa Region, South of Ukraine. The prevalence of iron deficiency anaemia was most seen in case of football having 46.7% of the cases out of the total diagnosed with the disorder.
Results and Data of Participants Diagnosed with the Disorder: (All necessary Permissions and Consent have been obtained from these participants for the release/sharing of this data)
Iron Deficiency Anemia in Athletes: Prevention, Management & Treatment:
🔹 Preventive Measures
• Iron-rich diet: Red meat, fish, poultry, lentils, tofu, leafy greens, fortified cereals.
• Enhance absorption: Take with Vitamin C-rich foods (citrus, tomatoes).
• Avoid inhibitors: Limit tea, coffee, calcium, and high-fiber foods near meals.
• Regular monitoring: Hemoglobin, ferritin, and transferrin saturation—especially for endurance athletes.
• Training load: Avoid overtraining; high-impact sports can cause blood loss (e.g., foot-strike hemolysis).
• Menstrual management: Female athletes may need extra iron or medical guidance for heavy periods.
🔹 Management
• Early recognition: Look for fatigue, breathlessness, poor performance, frequent infections.
• Nutrition consult: Balanced, iron-sufficient diet plan is key.
• Supplement decision: Ferritin <30 ng/mL may require iron supplements, even with normal Hb.
• Address causes: GI blood loss, poor intake, menstruation, or chronic inflammation.
• Altitude training: Increases iron needs—consider supplementation.
🔹 General Treatment
(Need to be sure to consult respective Doctors/Physicians as dose, preparations may vary person to person taking in account the medical history of patient)
• Oral iron: Ferrous sulfate 325 mg (65 mg elemental iron), 1–2 tabs/day. Take with Vitamin C, on empty stomach.
o Side effects: GI upset—can switch to gentler forms (e.g., ferrous bisglycinate).
• IV iron: For severe cases, malabsorption, or intolerance to oral iron (e.g., iron sucrose, ferric carboxymaltose).
• Duration: Continue 3–6 months post-correction to replenish stores.
• Follow-up: Recheck Hb & ferritin after 6–8 weeks of therapy.
|